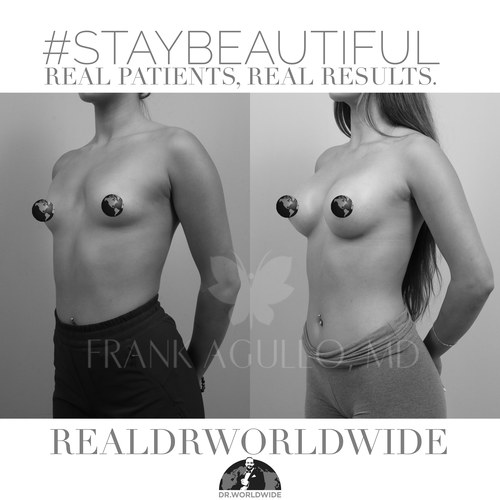
A woman sat in my consult room last week, pulled up a photo of herself at twenty-five, and said the line I hear several times a week. She wanted the fullness she used to have, and she wanted to know why she should drive past three closer surgeons to see me.
Here is the honest answer. For most augmentations I do now, I never touch the muscle. Not minimally. Not partially. Not at all.
That is a bigger deal than it sounds, and it is the reason recovery looks nothing like what your mother or your older sister went through.
What the Preserve Actually Is
The Preserve augmentation is prepectoral. The implant sits in front of the pectoralis muscle and behind your breast gland, above the muscle but below the gland. I do not cut the muscle, release it, or go under it.
That distinction is everything. A traditional submuscular augmentation goes behind the pectoralis and partially releases it off the chest wall. That release is the source of the long, sore, six-to-eight-week recovery patients remember. Preserve never goes there, so that whole chapter disappears.
I make the pocket by balloon dissection. No cutting, no electrocautery. The tissues are pushed outward, and the pocket is defined by your breast’s own ligaments. Those ligaments hold the implant in position, which is why I do not need mesh to support it.
That also means the nerves and arteries stay where they belong. You keep a higher likelihood of preserving sensation and breast function, because I am not dividing the structures that supply them.
Preserve Versus Traditional, Side by Side
| Question | Traditional Submuscular | Preserve Prepectoral |
|---|---|---|
| Where the implant sits | Behind the muscle | In front of the muscle, behind the gland |
| Is the muscle cut | Yes, partially released | No, never touched |
| How the pocket is made | Cutting and cautery | Balloon dissection |
| What holds the implant | Muscle and capsule | Your own ligaments |
| Typical recovery | Six to eight weeks | Back to work in one to three days |
How I Pick Your Size
Cup size is a starting point, not a measurement. I work from your dimensions and a Chrysalix 3D simulation, not from a letter on a bra tag.
Almost everyone has some asymmetry, and that is normal. Breasts are sisters, not twins. So I will often choose slightly different volumes on each side to get you closer to even.
There is a quieter advantage to placing above the muscle. I can put the implant precisely where your breast needs the most volume instead of filling the whole breast uniformly. A smaller implant can give a larger apparent size and a little lift. Lighter breast, same result you wanted.
The Implants I Use, and the Ten-Year Myth
I use Motiva Ergonomix. The old rule about swapping implants every ten years does not apply to these. The rupture rate is under half a percent, and they carry a lifetime guarantee.
The surface matters too. These use a nano-surface called SmoothSilk, which produces the lowest inflammatory response of any implant on the market and an extremely low capsular contracture risk. They are soft, the gummy bear type, and they take on a natural teardrop shape when you stand. Ergonomix implants move with the body, so you do not get that fixed, stuck-on look.
What Recovery Honestly Looks Like
This is the part that surprises people, so I will be specific.
I do it under light conscious sedation. You breathe on your own, and you will not remember much. I place Exparel, a long-acting local, between the ribs so the breast stays numb for about the first three days. The incision is two and a half to three centimeters in the fold under the breast, hidden where you will not see it.
The implant placement takes about thirty minutes. Patients are usually awake, pain-free, and able to raise their arms overhead before they leave, often within an hour. Many go back to work the next day, and the gym is reasonable at about two weeks if augmentation is the only thing we did. Add a lift or liposuction and the timeline shifts, and I will tell you that up front.
Why I Was One of the First to Do This
Being an early adopter of Preserve was a deliberate choice. Motiva trained me directly as one of roughly twenty highly selected surgeons in the United States, and I traveled to Costa Rica twice for that training. There are still fewer than forty surgeons in the country doing this.
I am a double board-certified plastic surgeon, certified by the American Board of Plastic Surgery and the American Board of Surgery. I completed my plastic surgery fellowship at the Mayo Clinic and I teach as a Clinical Associate Professor of Plastic Surgery at Texas Tech University Health Sciences Center Paul L. Foster School of Medicine. I committed to preserving your own anatomy because it recovers faster and ages better than cutting through muscle ever did.
The Animation Problem You Avoid
Here is a detail patients rarely hear about until it bothers them. With a traditional submuscular implant, every time you contract your chest, the muscle squeezes the implant and the breast moves or distorts. Surgeons call it animation deformity, and it is a direct consequence of putting the implant under a muscle that is built to move.
Preserve sidesteps it entirely, because the implant never goes under the muscle. You can do a push-up, a plank, or a heavy press without watching your breast jump. For an athlete, a CrossFit patient, or anyone who lifts, that is not a small thing, and it is one of the quieter reasons I prefer this plane.
One Honest Caveat
Preserve is not for absolutely everyone. Very thin patients with almost no breast tissue sometimes need a different plan, and I will say so in the room rather than force the technique. If a standard augmentation or a fat-based approach fits you better, that is the conversation we have.
Read the Patient-Facing Versions
For the patient-facing walkthrough, see the companion post on agulloplasticsurgery.com. For the practice overview, see the version on swplasticsurgery.com.
Ready to Talk?
The honest answer to what size and which implant is right for you needs an exam and a 3D simulation. Come see me.
Call the office at (915) 590-7900, text 1-866-814-0038, or book online at agulloplasticsurgery.com. #StayBeautiful.
@RealDrWorldWide on Instagram, TikTok, and Snapchat, @Agullo on X, or @AgulloPlasticSurgery on Facebook.