Saturday night, Stephanie Han defended her WBA lightweight world title against Holly Holm at the El Paso County Coliseum, live on ESPN, and won by decision. She is 13-0. About four months earlier, she was on my operating table for a breast augmentation, and nobody in her camp knew.
We sat down together to talk through how that was possible. Our conversation is below, in her words and mine.
Your Body Is Your Livelihood. Why Did You Decide to Do This?
Stephanie: “It’s something I’ve wanted to do for a very long time, and I always held back because of the stigma, that you shouldn’t do it because it’s going to affect your performance as a professional fighter. But I did my own research and realized I can still perform at an elite level. Most importantly, I’m doing it for myself. I don’t ask for a lot of things in life. This is personal.”
You’re a Mom of Two Who Breastfed Both. How Did That Factor In?
Stephanie: “I’m a mom of two beautiful kids, and I breastfed both of them. No one tells you your breasts won’t be the same afterward. I could train, I could do a million push-ups, and it would not change this. This was probably my biggest insecurity. I knew if I got it done, it would boost my confidence and make me feel comfortable in my own skin again.”
What Makes Motiva Preservé Recover So Differently?
Dr. Agullo: It comes down to where the implant sits and how we get there. We make a small incision in the fold, about two and a half centimeters, and we open the pocket above the muscle, behind the breast gland. There is no cutting and no electrocautery. We use a balloon to create the space, so we are just pushing the tissues outward and letting the breast’s own ligaments hold the implant. We preserve the nerves and the arteries, and because the muscle is never released, the recovery is fast. We do not even need a mesh. Most patients are back to work the next day and back in the gym in about two weeks.
Her Implants Were Not a Matched Pair, Were They?
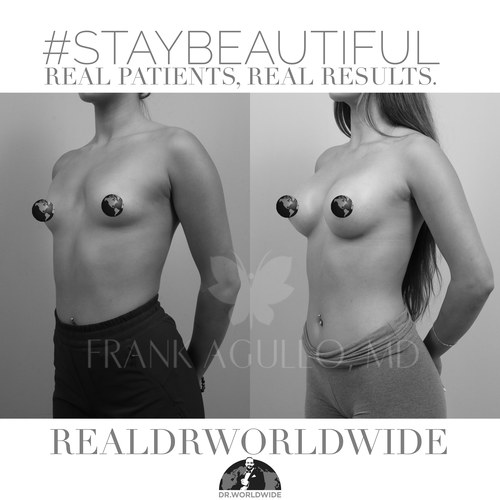
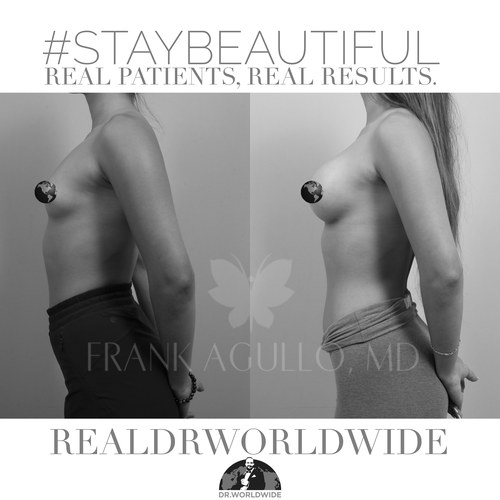
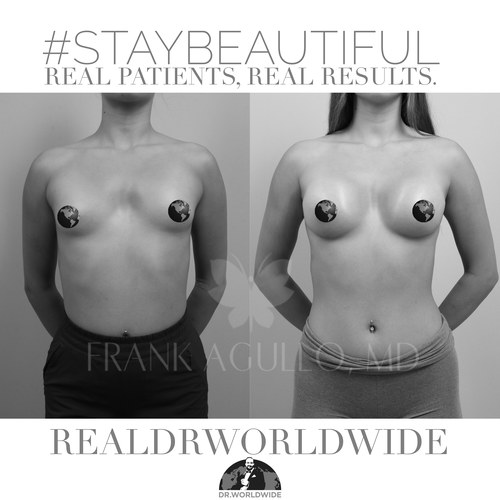
Dr. Agullo: No, and that is part of the artistry. Stephanie had a meaningful difference between the two sides, which is very typical, since we all have an asymmetric side. On the 3D simulation we planned a 265cc Demi Ergonomix on the right, with a little less projection, and a 315cc Full Ergonomix on the left. The Ergonomix implants move with the body, so they fill in beautifully and read as symmetric, even when she cuts weight for a fight.
What Was the Recovery Actually Like?
Stephanie: “Dr. WorldWide told me I’d be fully recovered in two weeks, and honestly I didn’t believe it until it happened. I had maybe a little discomfort for about three days, and after that it felt amazing. It’s been about four months and it truly feels like I didn’t get them done.”
Back in Camp Four Months Later. How Did Your Body Hold Up?
Dr. Agullo: I was surprised she never told her coach, but it made for a perfect test, because he was blinded to it. He watched her spar and train for the whole camp and thought she was in the best shape he had ever seen. That tells me the augmentation did not get in the way of her performance, her strength, or her range of motion, which is exactly the point of Preservé.
Stephanie: “Today I sparred 12 rounds and there was no pain. I can run seven miles, no problem. It feels like nothing, like they’re not even there. It’s maybe a pound of extra weight, and it feels like part of my body.”
Does That Mean the Surgery Helped Her Performance?
Dr. Agullo: No. The implants did not make her a better fighter. They boosted her confidence enormously, she does not stop talking about them, but they did not change her fighting. The whole point is that they did not affect it. They did not make her worse. That is what makes this such a good illustration of what the procedure can do for athletes, and really for all women.
How Do You Feel About the Result?
Stephanie: “They’re so symmetrical, so nice and perky. It’s taken my confidence from probably a six to a ten. I feel beautiful, I feel strong, I feel confident. And at the end of the day, I’m still Stephanie Han. I’m still a world champion boxer, still a police officer, still a mother of two, still a woman of God. This doesn’t change who I am. It’s just something I wanted for myself.”
Is This the Recovery Every Patient Should Expect?
Dr. Agullo: It is realistic for most women having Preservé on its own. Back to work within one to three days, back in the gym at about two weeks, the way I have seen with many patients. If a patient also needs a lift, or is having liposuction or a mommy makeover with a tummy tuck, that changes everything, and the recovery is dictated by those other procedures. For the full breakdown of the technique, the implant, and the recovery ladder, I wrote that up in Back to the Gym in Two Weeks: Motiva Preservé and What Preservation Surgery Actually Means. The technique itself is on the Motiva Preservé page at agulloplasticsurgery.com, and the broader breast augmentation overview is on swplasticsurgery.com.
What Would You Tell a Woman Who Has Been Holding Back?
Stephanie: “This is one of the things I do not regret at all, and I honestly wish I’d done it sooner. Don’t listen to the stigma. You can still be strong, you can still be beautiful, and you can still perform at 100 percent. To every mom and every athlete, especially the women champion boxers and the moms who breastfed, if you have two weeks, you can do it.”
Ready to Talk?
If Stephanie’s story sounds like the version you want, the next move is a consultation. I will tell you whether Motiva Preservé fits your anatomy and your goals, and I will give you a recovery timeline I can actually defend. The goal is the body you recognize in the mirror, and a recovery you can plan your life around. #StayBeautiful.
Call (915) 590-7900, text 1-866-814-0038, or book online at agulloplasticsurgery.com. Follow along at @RealDrWorldWide on Instagram, TikTok, and Snapchat, @Agullo on X, or @AgulloPlasticSurgery on Facebook.